
Causes of Obesity

Energy Balance in the Development of Obesity
Obesity can result from a minor energy imbalance, which lead to a gradual but persistent weight gain over a considerable period. Some researchers have hypothesized that energy imbalance is the result of inherited metabolic characteristics; whereas others believe it is caused by poor eating and lifestyle habits, that is “gluttony and sloth”.
Positive energy balance occurs when energy intake is greater than energy expenditure and promotes weight gain (Figure 4). Conversely, negative energy balance promotes decrease in body fat stores and weight loss. Body weight is regulated by a series of physiological processes, which have the capacity to maintain weight within a relatively narrow range (stable weight). It is thought that the body exerts a stronger defence against under nutrition and weight loss than it does against over-consumption and weight gain.
Figure 4 also suggests that positive energy balance and weight gains are influenced by powerful societal and environmental forces which may overwhelm the physiological regulatory mechanisms that operate to keep weight stable. These include increasing automation, lack of recreational facilities and opportunities, increase in food variety and availability. Moreover, the susceptibility of individuals to these influences is affected by genetic and other biological factors such as sex, age and hormonal activities, over which they have little or no control (WHO 1998).
Dietary intake and physical activity are important contributing factors in the development of obesity. If calorie intake is in excess of requirement it will be stored mainly as body fat (Figure 4). If the stored body fat is not utilised over time, it will lead to overweight or obesity.
Inter-individual variations in energy intake, basal metabolic rate, spontaneous physical activity, the relative rates of carbohydrate-to-fat oxidation, and the degree of insulin sensitivity seem to be closely involved in energy balance and in determining body weight in some individuals (Ravussin 1993).

Factors that promote or protect against weight gain
WHO (2003) examined the various aetiological factors that could lead to unhealthy weight gain. These factors were categorised based on strength of evidence, namely convincing, probable, possible and insufficient as shown in Table 8.

Dietary Intake
Food consumption pattern
Dietary patterns of Malaysians have changed markedly, as evidenced from an analysis of food availability in the past four decades (1960s – 2000). Although these data should not be equated with consumption levels, food balance sheet data are useful in indicating probable trends in food consumption patterns. In the absence of regular food consumption surveys, these data do provide some useful information, within the recognized limitations of such data (Tee 1999).
FAO Food balance sheet data have shown that there has been a trend of increasing per capita availability of the major macro nutrients calories, fat and protein, particularly theformer two nutrients (Figure 5). There was also a steady increase in the proportion of the calories from animal sources from 10% in the 1960s to 20% in the late 1990s. In the case of protein, proportion from animal sources also increased from 30% to almost 60% during the same time period. The increase in proportion of fat from animal sources was not so dramatic.

The changes in the sources of available calories are shown in Figure 6. A steady decline in calories from complex carbohydrates, notably cereals, is evident, from 60% in the 1960s to 40% in mid 1990s and appeared to have remained at that level. The availability of other fibre-rich foods, such as fruits and vegetables, has not increased over the years. There was a concomitant increase in the proportion of calories from oils and fats, sugars and meat, fish and eggs.
Similar changes in sources of available protein can be seen in Figure 7. The proportion
of protein from cereals and from meat, fish and egg appeared to have levelled off in the
late 1990s.


Figure 8 shows the percentage contribution of the three main nutrients namely carbohydrates, fat and protein to the total available energy over the past four decades. There has been a definite decline in the proportion of energy from carbohydrates, from about 73% in the 1960s to about 63% in 2000. At the same time, the percentage contribution of fat was observed to have increased from 18% to 27% .

Local food consumption studies amongst different population showed that dietary energy intake varies widely. The contribution of fat ranges from 20 to 30 percent of total calories and tends to be higher among urban population. However, it should be borne in mind that dietary intake is not the only factor contributing to obesity.
Macronutrient composition of the diet
The association between energy intake and body weight relies on the ease with which excess macronutrients can be deposited as adipose tissue. The energy cost of nutrient storage is not identical for all macronutrients. The cost of fat storage from dietary fat is the lowest, followed by carbohydrate and protein (Flatt 1978). Macronutrients with a low storage capacity such as protein and carbohydrate will be preferentially oxidized when intakes exceeded requirements. Hence, excess dietary fat is more likely to be stored in the body and this capacity is unlimited (Astrup et al. 1994; Horton et al. 1995). The caloric content of fat is also more than twice that of protein or carbohydrate (Table 9).

Alcohol is not stored in the body thus all ingested alcohol is oxidized immediately. This response dominates oxidative pathways and suppresses the rates at which other fuels are oxidized. The obligatory disposal of alcohol will promote fat storage because it operates at the expense of fat oxidation (Suter et al. 1992).
In summary, after a meal the body has a specific order in which it burns up the fuels, that is, alcohol, followed by protein then carbohydrate and finally fat.
Table 10 highlights the main characteristics of the macronutrients of which fat seems to be the key macronutrient which undermines the body’s weight regulatory systems since it is very poorly regulated at the level of both consumption and oxidation. As yet there is no consensus regarding the role of sugar intake on body weight regulation, but there is some concern that the over consumption of sweet-fat foods (such as chocolate bars, ice cream, cream puff) may be a problem in a subgroup of the population. Although high protein intakes may appear to be advantageous in controlling energy intake and contributing to good body weight regulation, high protein intakes (especially animal protein) have been associated with some adverse health consequences such as renal disease, cancer and cardiovascular diseases (WHO 1998). These probably due to the fact that some animal protein foods are also associated with high fat and cholesterol contents

High fat diets
Foods or meals that are high in fat are smaller in weight or volume than highcarbohydrate foods or meals of similar energy content (SIGN 1996). Dietary fat content is directly correlated with energy intake, produces only weak satiation in comparison with protein and carbohydrate, and is thought to be processed efficiently by the body. A number of studies found that individuals on a high-fat diet are more prone to become overweight (Popkin et al. 1995).
Drewnowski and Popkin (1997) reported that irrespective of income, fat availability has increased in Asia between the years 1975 to 1994 and more so in the affluent society (Figure 9).

Energy dense foods and drinks
Consuming too much or too often high calorie foods and drinks may increase the total calories and thus result in obesity (SIGN 1996). Examples of commonly eaten high calorie Malaysian foods are given in Appendices A3 and A4. They are mostly deep-fried or cooked with santan (coconut milk).
The energy density of foods may be contributed by its macro nutrient contents. A high fat food will often be labelled as energy-dense. However, sugars for example table sugar, honey, syrups also contribute to energy density. Extra sugars added to low fat confactionaries, kuih, cakes or desserts will increase the calorie content of the food (Appendix A4). Low fat food products may also be high in calories and therefore should not be eaten in excess. Beverages containing substantial amounts of sugar or alcohol can also contribute to excessive calorie intake. Consumers are encouraged to read and compare food labels to make healthy choices (Appendix A5).
Fibre content in the diet
A diet with adequate amounts of fibre-containing foods is usually less energy dense. Its greater bulk has a short-term satiety effect, can help to prevent overeating and reduce risk of obesity (WHO 2003). The Malaysian Recommended Nutrient Intakes (NCCFN 2005) recommends an intake of 20 to 30 grams of dietary fibre per day. This can be achieved by including fruits, vegetables, whole grain cereals, pulses and legumes in the diet. Efforts to increase dietary fibre intake should be gradual to minimize discomfort such as bloating and flatulence. It is important to drink a lot of water when increasing fibre intake.
Food palatability
Palatability is defined as the momentary subjective orosensory pleasantness of a food, which indicates the sensory stimulation to eat. It is one of the most powerful influences in promoting calorie over-consumption (positive energy balance) by increasing both the rate of eating and the sense of hunger during and between meals. Perceived palatability of foods plays a major role in determining which foods are selected over others (Drewnowski & Popkin 1997). It has also been argued that palatability is associated with the energy density of foods. Foods that are energy dense are more palatable than those of lower energy density (Drewnowski 1998). Fat is associated with palatability and pleasurable mouth-feel that can induce behaviour which favours over-consumption (Blundell & King 1996) leading to obesity.
Sweetness is another powerful, easily recognized and pleasurable taste. Thus, many foods are sweetened in order to increase their palatability and consumption. However, consumption of sugars leads to a subsequent suppression of energy intake approximately equivalent to the amount provided by sugars (Mazlan 2001). Nevertheless, sweetened foods that have a high fat content are expected to be conducive to excess energy consumption since palatability is enhanced by both sweetness and mouth-feel, and fat has only a small suppression effect on appetite and intake. Both fat and sugar increase palatability of foods and thus help to promote overeating.
Unhealthy dietary practices
In Malaysia, a changing environment and increasing affluence have widened food
options and changed eating habits. Groceries and supermarkets stock their shelves with a
greater selection of foods. Fast foods and soft drinks which are high in calories, from
either fat or sugar, are more accessible (Ismail 2002). It is also becoming a trend that
more restaurants are extending their business hours to late night or to 24 hours
Causes of Obesityencouraging late night suppers. Malaysians may be eating more during a meal or snack because of larger portion sizes. People who frequently skip meals, especially breakfast, are more likely to overeat at other times. All of these are unhealthy dietary practices that would result in excessive energy intake and thus overweight problems.
Other unhealthy dietary practices that lead to obesity include binge eating, which if uncontrolled can escalate into binge eating disorder (BED). BED is defined as eating large amounts of food while feeling a loss of control over their eating behaviour. Among mildly obese people, 10 to 15 percent have binge eating disorder and this disorder is even more common among those with severe obesity (de Zwaan & Mitchell 1992).
Energy Expenditure
Total energy expenditure has three main components, namely, basal metabolic rate (BMR), thermogenesis or thermic effect of food (TEF) and physical activity (Figure 4). Basal metabolic rate is the energy expended by a person who is fasting and at rest in the morning under comfortable ambient conditions. The BMR includes the cost of maintaining the integrated system of the body and in most sedentary adults; BMR constitutes about 60% to 70% of the daily energy expenditure. Although the BMR may vary intrinsically by ±25% between individuals of similar weight, within each individual it is tightly controlled (Dallosso & James 1984). Hence, the key variable of energy output in an individual is the degree of physical activity. In a dynamic phase, in which an individual gains weight as a result of energy intake exceeding energy expenditure over a prolonged period, BMR will increase due to the larger fat-free mass (including that of the expanded adipose tissue) as well as to an additional energy cost of activity imposed by the extra weight (Diaz et al. 1992).
The BMR of adult Malaysians were 10-13% lower than the BMR estimated using the FAO/WHO/UNU (1985) equations but only differed by 3% when compared with Henry & Rees (1991) equations for population in the tropics (Ismail et al. 1998). On the other hand, Poh et al. (1999) found that BMR values predicted from the FAO/WHO/UNU (1985) equations overestimated the BMR of Malaysian boys by 3% and that of girls by 5%, while the Henry & Rees (1991) equations for populations in the tropics underestimated BMR of boys and girls by 1% and 2%, respectively.
Thermogenesis is the increase in basal metabolic rate in response to stimuli such as food intake, cold or heat exposure, psychological influences such as fear or stress, or the administration of drugs or hormones. The thermic effect of food (the major form of thermogenesis) accounts for approximately 10% of the total daily energy expenditure.
Physical activity is the most variable component of daily energy expenditure, which may account for a significant number of calories in very active individuals. Sedentary adults however, exhibit a range of physical activity that still represents about 20% to 30% of the total calorie expenditure.
Physical Activity
Modern life is becoming increasingly sedentary and has been associated with an increased risk of obesity. Most modern jobs can be carried out with less physical effort due to technical progress, urbanization, transport and availability of a large range of domestic electrical appliances resulting in substantial decline in the energy spent in these activities. Recent studies (Table 11) in different age groups suggest that with the exception of armed forces and elite athletes, Malaysians are also leading a sedentary lifestyle (Ismail 2002). Physical activity level (PAL) values express daily energy expenditure as multiples of BMR.

There is convincing evidence that regular physical activity is protective against unhealthy weight gain whereas sedentary lifestyles, particularly sedentary occupations and inactive recreation such as watching television, promote it (WHO 1998).
Definition
The definition of physical activity and physical inactivity (sedentary behaviour) has been reported in the WHO 1998 Report.
Physical activity is defined as any bodily movement produced by skeletal muscles that result in a substantial increase over the resting energy expenditure (Bouchard et al. 1994). It has three main components:
(i) Occupational work - activities undertaken during the course of work
(ii) Household and other chores - activities undertaken as part of day-to-day living
(iii) Leisure-time physical activity - activities undertaken in the individual’s discretionary or free time.
Activity is selected on the basis of personal needs and interest. It includes exercise and sports.
a. Exercise - a planned and structured subset of leisure-time physical activity that is usually undertaken for the purpose of improving or maintaining physical fitness
b. Sports - its definition varies around the world. It implies a form of physical activity that involves competition and also embraces general exercise and a specific occupation.
Physical inactivity, or sedentary behaviour as it is otherwise known, can be defined as “a state when body movement is minimal and energy expenditure approximates resting metabolic rate” (Dietz 1996).
However:
• Physical inactivity represents more than an absence of activity; it refers also to participation in physically passive behaviours such as television viewing, reading, working at computer, talking with friends on the telephone, driving a car, meditating or eating (Ainsworth et al. 1993).
• Physical inactivity may contribute to weight gain through other means than reduction in energy expenditure. For example, recent studies in adolescents (Lytle et al. 1995) and adults (Simoes et al. 1995) have demonstrated significant relationships between inactivity and other adverse health practices, such as the consumption of less-healthy foods and an increased fat intake.
The decline in energy expenditure seen with modernization and other societal changes is associated with a more sedentary lifestyle in which motorized transport, mechanized equipment, and labour-saving devices both in the home and at work have replaced physically arduous tasks (Table 12).
Physical activity and the resting metabolic rate (RMR)
As explained in Section 5.3, basal metabolic rate (BMR) is the amount of energy the body needs to function while at rest. This energy is used to keep the heart beating, temperature regulated, and other organs functioning. Basal metabolic rate is measured under very restrictive circumstances. On the other hand, resting metabolic rate (RMR) is a more common and closely related measurement, measured under less strict conditions.
The effect of physical activity in increasing RMR has not been totally resolved. Several cross-sectional studies have found that highly trained runners have higher RMRs than untrained people of similar age and size. But other studies have not been able to confirm this (Poehlman 1989). Few longitudinal studies have showed that RMR might increase following training, but the data are not conclusive (Broeder et al. 1992). Because RMR is closely related to the fat-free mass of the body (fat-free tissue is more metabolically active), interest has increased in the use of resistance training to increase fat-free mass in an attempt to increase RMR.

Physical activity level (PAL)
PAL values express daily energy expenditure as multiples of BMR, thereby allowing approximate adjustment for individuals of different sizes. PAL is a universally accepted way of expressing energy expenditure and help to convey an easily understandable concept.
Individuals whose occupation involves regular physical activity are likely to be at PALs of 1.75 or more. Individuals whose lifestyle involves only light occupational and leisure activity are likely to have PAL of 1.55 – 1.60. Some individuals who engage in no activity whatsoever will have PAL below this range, at around 1.40. In order to avoid obesity, populations should remain physically active throughout life at a PAL of 1.75 or more (Table 13).

Table 14 shows some ways in which PAL can be raised from 1.55 – 1.60 up to 1.75 or more by the equivalent of an extra hour of moderate activity each day. More strenuous activities require less time than one hour per day to bring the overall average daily PAL up to 1.75.

Long-term increases in population physical activity levels are more likely to be achieved through environmental changes. It is recommended to increase or maintain incidental daily activities and low-intensity leisure pursuits such as walking, climbing stairs and gardening rather than by encouraging occasional vigorous exercise.
For the prevention of unhealthy weight gain, recent recommendations (Saris et al. 2003) have suggested that current guidelines of 30 minutes of moderate activity, such as brisk walking and cycling, daily which is important for limiting health risks to chronic diseases is insufficient. In order to prevent weight gain or regain, compelling evidence suggest that 60 to 90 minutes of moderate activity are needed. In addition, it has also been suggested that to prevent transition to overweight and obesity, a PAL of 1.7, or approximately 45 to 60 minutes per day of moderate activity is necessary. For children even more time is recommended for physical activity.
Exercise and appetite
Woo & Pi-Sunyer (1982) showed that obese women did not compensate the higher energy expenditure induced by exercise with increased intake, and thereby obtained a significant negative energy balance on exercise. This suggests that those who have an excess amount of energy stored may particularly benefit from regular exercise. Hunger can be temporarily suppressed by intense exercise, and possibly by low-intensity exercise of long duration. Hence, there is no supporting evidence for the common perception that exercise stimulates appetite, leading to an increased food intake that even exceeds the energy cost of the preceding activities.
Health benefits of physical activity
Physical activity has been shown to improve the physiological aspects of our body system such as cardiovascular, respiratory, metabolic and weight control. There is convincing evidence that physical activity reduces risks of obesity, type 2 diabetes, CVD, certain cancers and osteoporosis.
Other benefits of physical activity includes becoming more energetic, improved selfesteem, increased resistance to stress, build stronger muscles and joints, increased fitness and flexibility, and living a healthier and longer independent life.
On the other hand, physical inactivity and sedentary lifestyle increase risk of obesity and type 2 diabetes (WHO 2003).
Psychosocial Factors contributing to Obesity
Introduction
Psychosocial factors take precedence in terms of contribution to obesity because genetic changes do not occur quick enough to warrant the increase of obesity cases around the world (Crawford & Ball 2002). Behaviour is governed by psychological aspects of human functioning, and is learnt through various experiences, including conditioning, reinforcements and modelling (Franken 1994). Calorie intake and use largely depend on behaviour, which are food-related and non-food related. The significance of behavioural factors in weight gain is that it can be modified more easily than genetics.
Hunger and appetite
Hunger is a physiological response to a need for food triggered by stimuli acting on the brain (Liebowitz 1995). It can be affected by a number of factors such as the size and composition of preceding meal, habitual eating pattern, exercise, physical and mental states (Franken 1994). In a normal eating pattern hunger begins after four to six hours after eating, when food has left the stomach and much of it has been absorbed by the body. This pattern is highly influenced by psychophysiological factors such as smell, as well as environmental interactions (French et al. 2001).
Individuals who restrict food consumption at each meal may feel extra hungry for a few days, but then hunger diminishes for a time. However, at some point of food deprivation, hunger can be uncontrollable and lead to bouts of overeating that more than make up for the calories lost. The stomach capacity can also adapt to larger food quantities and until a normal meal size no longer feel satisfying.
Appetite or subjective hunger also initiates eating, but unlike hunger, appetite is learned. Appetite intensifies hunger but an individual can experience appetite without hunger (Franken 1994). A good example is the effect of seeing and smelling food after finishing a big meal – despite an already full stomach, appetite is still strong. Appetite can be affected by factors such as learned preferences, timings of meal, environmental cues and social interactions (Blundell 1995).
At some point during a meal, the brain receives stimuli from several sources that enough food has been eaten. This process is called satiation (Franken 1994). A lack of satiety between meals can lead to overeating when a mealtime arrives. In some cases this sets up a cycle of starvation and binging, which lead to overeating. The choice of food may affect satiety – some foods seem to sustain satiety for longer period than others. In general foods high in protein and fibre sustain satiety longer than those high in fat or sugar.
Food-related behaviour
Humans have the ability to override signals of hunger and satiety and eat whenever they wish, especially when presented with circumstances that stimulate them to do so. Hence, overeating is a learnt process with regards to modelling, conditioning and habituation. The main behavioural factors that contribute to obesity include:
• excessive energy intake, and diminished rate of physical activity or energy output,
• greater responsiveness to stimuli associated to food (especially energy dense food),
• large bites of food and rapid eating – rapid eating allows greater amount of food to be consumed before satiety signals are recognised.
According to learning theories, certain types of food can be associated with certain pleasures, (e.g. eating while watching favourite TV program); or sets of personal beliefs, (e.g. the impropriety of wasting food). Furthermore, certain situations and circumstances (i.e. time of the day, food court, mere presence of food, emotions/mood state) are associated with certain foods or eating response, thus creating the craving for food. Therefore, such situations may lead to patterns of overeating.
Learning theories also state that an eating behaviour is reinforced or strengthened when it is followed immediately by a pleasurable activity or experience. These reinforcers can be in the form of the positive psychological and physiological experience of satiety, pleasant taste (e.g. foods high in fat, salt or sugar), social approval or acceptance, and distraction from negative events (e.g. relationship problems). In addition to inducing an individual to eat more, these reinforcers also change behaviour dynamics in eating, such as bigger bites, eating faster and piling on food on the plate.
On the opposite of reinforcement, there is punishment, which is an unpleasant experience. For example, hunger is a discomforting feeling and can be categorised as punishment for not eating. As such, continuous eating can be shaped so as not to experience hunger, thus leading to overeating.
Overeating behaviour can also be modelled after. It can be used as a coping mechanism to deal with daily stressors, or as part of an accepted behaviour (e.g. serving food during meetings). Effect of modelling or imitation is greater when the behaviour is reinforced (Franken 1994). For example, watching others being praised for finishing a large amount of food, or for finishing a whole plate of a meal regardless of satiety level.
Non-food-related behaviour
Non-food-related behaviour can also lead to obesity. These behaviours are sedentary behaviours such as sitting or sleeping for long hours, using lifts as compared to stairwalking, driving to places that are within walking distance.
In the modern world, mechanisms that reinforces sedentary behaviours include comfort in not moving much, discomfort when walking in hot and humid conditions, rewards for inactivity (e.g. being able to play computer games, having pleasant discussion, pleasant sleep), and punishment for over activity, especially in children. Many sedentary lifestylepromoting factors such as the television, motorised transportation, computers and other labour-saving devices are increasingly available thus reducing the need for physical activity (French et al. 2001).
In today’s working world, the opportunities for physical activity seem to be decreasing as the current lifestyle trends seem to be more geared towards daily career work. Moreover, there is little availability or accessibility in recreation spaces for people to participate in regular physical activities (French et al. 2001). Therefore, there is little behavioural reinforcement for physical activities, thus encouraging more sedentary behaviours.
Culture
Culture certainly has a big influence on behaviours leading to weight gain. The concepts of personal well being such health, affluence, beauty, strength and prosperity are modelled and learnt from society at large (Matsumoto 1994). As such, culture and society that accepts overweight as favourable, would lead to behaviours that reinforces weight gain.
Behaviours that lead to weight gain are influenced at various social levels such as peer groups, parents, partners, friends and authority figures, or socio-economic environment. Social influence can be a very strong factor in eating behaviour and weight management.
It is usual that people tend to eat the foods that are eaten by their family and friends for reasons such as having a sense of acceptance and belonging, compliance to authority (i.e. parents, teachers, nutritionists, dietitians, etc.), as well as having consistencies in attitudes, beliefs and habits of diet and nutrition formed through learning within the community (Sobal 1995). Other social influence variables include gender roles (i.e. women tend to be fatter), life development (e.g. people tend to grow fatter as they age,and then decline), ethnicity, socio-economic status, parenthood (mothers tend to be heavier) and geographical location (Sobal 1995).
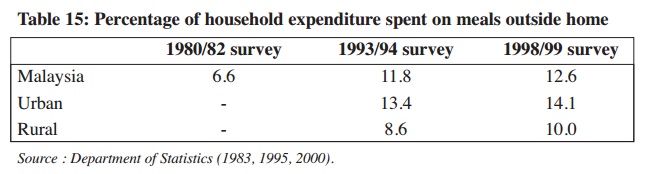
One such cultural influence with regards to socio-economic environment is eating out. Eating out has become popular as it is highly convenient for today’s modern household. Eating out at restaurants and eating food prepared away from home has been found to be increasing in trend in the past 20 years (French et al. 2001). Local data shows similar trend not only in the urban but also in the rural area (Table 15). Moreover, food prepared away from home tend to be larger in portion, as well as higher in fat and energy. This change in nutritional quality is a cause for concern as there is increasing intake of higher than needed energy consumption. Mass media influence plays a large role in eating out behaviour by exposing messages that encourage food consumption, which leads to the increase of food availability (French et al. 2001).
Personality factors and cognitive style
Personality style as well as thinking patterns can help maintain behaviour that leads to obesity. Feelings of hopelessness can demotivate individuals from reducing and maintaining weight (Byrne 2002). On the contrary, individuals with high self-acceptance are unlikely to change themselves either.
Coping styles, determine how individuals cope with daily as well as acute life stress-ors. Irrational thinking styles and poor problem solving skills usually lead to negative coping mechanisms that may involve behaviour that promotes weight gain (Byrne 2002). These include seeking food for comfort and reduction in activity (e.g. overeating and/or oversleeping when distressed). As such, psychological disorders, especially binge eating disorder (BED) could also lead to obesity. Research shows that binge eaters tend to have other psychiatric comorbidities such as personality, anxiety and mood disorders,especially lifetime episodes of depression (Marcus 1995).
REFERENCES
Ainsworth BE, Haskell WL, Leon AS, Jacobs DR, Montoye HJ, Sallis JF & Paffenbarger RS. (1993). Compendium of Physical Activities: Classification of energy costs of Human Physical Activities. Medicine and Science in Sports and Exercise; 25: 71-80.
Astrup A, Buemann B, Christensen NJ & Toubro S. (1994). Failure to increase lipid oxidation in response to increasing dietary fat content in formerly obese women. American Journal of Physiology. 266:E592-E599.
Blundell JE. (1995). The psychobiological approach to appetite and weight control. In Brownell KD & Fairburn CG. (Eds.) Eating disorders and obesity: a comprehensive handbook. New York: Guilford Press. pp. 13-20.
Blundell JE & King NA. (1996). Overconsumption as a cause of weight gain: behavioural-physiological interactions in the control of food intake (appetite). In. The origins and consequences of obesity. (Ciba Foundation Symposium 2001). Chichester: Wiley.
Broeder CE, Burrhus KA, Svanevik LS & Wilmore JH. (1992). The effects of either highintensity resistance or endurance training on resting metabolic rate. American Journal of Clinical Nutrition. 55(4):802-10.
Bouchard C, Shepard RJ & Stephens T. (1994). Physical activity, fitness and health: International proceedings and consensus statement. Champaign, Il: Human kinetics Byrne SM. (2002). Psychological aspects of weight maintenance and relapse in obesity. Journal of Psychosomatic Research. 53:1029-1036.
Crawford D & Ball K. (2002). Behavioural determinants of the obesity epidemic. Asia Pacific Journal of Clinical Nutrition. 11(Suppl):S718-S721.
Dallosso HM & James WPT. (1984). The role of smoking in the regulation of energy balance. International Journal of Obesity. 8:365-375
Department of Statistics. (1983, 1995, 2000). Reports on household expenditure surveys for 1980/82, 1993/94 and 1998/99.
de Zwaan MD & Mitchell JE. (1992). Binge eating in the obese. Annals of Medicine. 24:303-308.
Diaz EO, Prentice AM, Goldberg GR, Murgatroyd PR & Coward WA. (1992). Metabolic response to experimental overfeeding in lean and overweight healthy volunteers. American Journal of Clinical Nutrition. 56:641-655.
Dietz WH. (1996). The role of lifestyle in health: the epidemiology and consequences of inactivity. Proceedings of the Nutrition Society. 55:829-840.
Drewnowski A. (1998). Energy density, palatability, and satiety: implications for weight control. Nutrition Reviews. 56:347-353.
Drewnowski A & Popkin BM. (1997). The nutrition transition: new trends in the global diet. Nutrition Reviews. 55(2):31-43.
FAO. (1961-2001). Food Balance Sheets. FAO website: http://apps.fao.org/faostat. Food and Agriculture Organization of the United Nations, Rome.
FAO/WHO/UNU. (1985). Energy and protein requirements. Technical Report Series 724. Geneva: World Health Organization.
Flatt JP. (1978). Biochemistry of energy expenditure. In: Bray G. Ed. Recent advances in obesity research. Westport: Techonomic.
Franken RE. (1994). Human motivation. 3rd Ed. Pacific Grove: California: Brooks/Cole.
French SA, Story M & Jeffery RW. (2001). Environmental influences on eating and physical activity. Annual Review of Public Health, 22, 309-335.
Henry CJK & Rees AG. (1991). New predictive equations for the estimation of basal metabolic rate in tropical people. European Journal Clinical Nutrition, 45:177-185.
Horton TJ, Drougas H, Brachey A, Reed GW, Peters JC & Hill JO. (1995). Fat and carbohydrate overfeeding in humans: different effects on energy storage. American Journal of Clinical Nutrition. 62:19–29.
Ismail MN, Ng KK, Chee SS, Roslee R & Zawiah H. (1998). Predictive equations for the estimation of basal metabolic rate in Malaysian adults. Malaysian Journal of Nutrition, 4:81-90.
Ismail MN. (2002). The nutrition and health transition in Malaysia. Public Health Nutrition; 5(1A): 191-195
Liebowitz SF. (1995). Central physiological determinants of eating behaviour and weight. In Brownell KD & Fairburn CG. (Eds.) Eating disorders and obesity: a comprehensive handbook. New York: Guilford Press. pp. 3-7.
Lytle LA, Kelder SH, Perry CL & Klepp K. (1995). Covariance of adolescent health behaviours: the class of 1989 study. Health Education Research. 10:133-146.
Marcus MD. (1995). Binge-eating and obesity. In Brownell KD & Fairburn CG. (Eds.) Eating disorders and obesity: a comprehensive handbook. New York: Guilford Press. pp. 441-444.
Matsumoto D. (1994). People: Psychology from a cultural perspective. Pacific Grove: Brooks/Cole Publishing Company.
Mazlan N, Horgan G & Stubbs RJ. (2001). Mandatory snacks rich in sugar, starch or fat: effect on energy and nutrient intake. International Journal of Obesity. 25(Suppl 2): S54.
NCCFN. (2005). Recommended Nutrient Intakes for Malaysia. Areport of the Technical Working Group on Nutritional Guidelines. Putrajaya: National Coordinating Committee on Food and Nutrition, Ministry of Health Malaysia.
Paul AA & Southgate DAT. (1978). McCance and Widdowson's the composition of foods. 4th ed. London: Her Majesty's Stationery Office.
Poehlman ET. (1989). A review: exercise and its influence on resting energy metabolism in man. Med Sci Sports Exercise. 21:515-525.
Poh BK, Ismail MN, Zawiah H & Henry CJK. (1999). Predictive equations for the estimation of basal metabolic rate in Malaysia adolescents. Malaysian Journal of
Nutrition. 5:1-14.
Popkin BM, Paeratakul S, Zhai F & Ge K. (1995). Areview of dietary and environmental correlates of obesity with emphasis on developing countries. Obesity Research. 3(Suppl. 2):145s–153s.
Ravussin E. (1993). Energy-metabolism in obesity - studies in the Pima Indians. Diabetes Care. 16(1):232-238.
SIGN. (1996). Obesity in Scotland: Integrating prevention with weight management. Edinburgh: Scottish Intercollegiate Guidelines Network.
Saris WH, Blair SN, van Baak MA, Eaton SB, Davies PS, Di Pietro L, Fogelholm M, Rissanen A, Schoeller D, Swinburn B, Tremblay A, Westerterp KR & Wyatt H. (2003). How much physical activity is enough to prevent unhealthy weight gain? Outcome of the IASO 1st Stock Conference and consensus statement. Obesity Reviews. 4 (2):101-114.
Simoes EJ, Byers T, Coates RJ, Serdula MK, Mokdad AH & Heath GW. (1995). The association between leisure-time physical activity and dietary fat in American adults. American Journal of Public Health. 85: 240-244
Sobal J. (1995). Social influences on body weight. In Brownell KD & Fairburn CG. (Eds.) Eating disorders and obesity: a comprehensive handbook. New York: Guilford Press. pp. 73-77
Suter PM, Schutz Y & Jéquier E. (1992). The effect of ethanol on fat storage in healthy subjects. New England Journal of Medicine. 326: 983–987.
Tee ES (1999). Nutrition of Malaysians: where are we heading? Malaysian Journal of Nutrition. 5(1&2):87-109.
Woo R & Pi-Sunyer FX. (1982). Effect of increased physical activity on voluntary intake in lean women. Metabolism. 34:836-841.
WHO. (1998). Obesity: Preventing and managing the global epidemic.Report of a WHO Consultation on Obesity. Geneva: World Health Organisation.
WHO. (2003). Diet, nutrition and the prevention of chronic diseases. Report of a Joint WHO/FAO Expert Consultation. WHO Technical Report Series 916, Geneva: World
Health Organisation.
About the author
 Admin
Admin
Obesity Awareness program is a cause that trying to promote and create awareness upon the citizen of Malaysia to maintain a healthy lifestyle. Organize in the fulfillment of New Media and Technology subject course requirement FKPM










0 comments: